Points to Pay Attention to in Neural Therapy Injections - First of all, care must be taken to…

For injections to be carried out as safely as possible, the patient should be in a comfortable but safe position.
A position should be chosen that does not require repositioning the patient differently for each injection and that does not create discomfort for the patient.
From the perspective of the physician performing neural therapy, the most important point is to reach the target by preferring, as much as possible, standardized positions for injections.
The supine (dorsal) position is suitable for all injections in the front (ventral) and side (lateral) areas of the body.
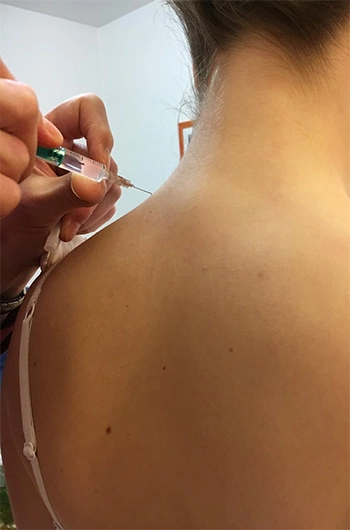
For injections on the back of the body, from the head area to the tailbone, a comfortable sitting position on the examination table should be preferred, while for injections made to the dorsal sections of the lower extremity, the lateral position should be preferred.
DISINFECTION
As a basic rule, the skin should be disinfected before every injection.
However, according to practical experience with procaine, it is known that in cases where the disinfection time is not observed, there is no increase in the incidence of injection-related infection.
Injections made to joints and to peridural spaces where the risk of dural damage is low must absolutely be carried out under aseptic conditions. The risk of infection at the injection site is very low, due to the strong perfusion-enhancing effect of diethylaminoethanol.
INJECTION APPLICATION IN NEURAL THERAPY
Every injection should be performed as painlessly as possible. It is recommended that every injection be performed, as much as possible, with a freely supported hand. In injections performed without support, there can be a risk of injecting into the wrong location and of injury to the patient.
To reach the correct injection site, a light pressure is applied to the plunger to slowly advance the cannula, resulting in a low degree of simultaneous infiltration for the different tissue types the cannula needs to pass through as it advances partly deeper (e.g., the paravertebral trunk, the prevertebral ganglion, the retroperitoneal space of the lesser pelvis).
 For this reason, the process becomes less painful for the patient. For this purpose, it is recommended to use replaceable, sharp, single-use cannulas that are as thin as possible.
For this reason, the process becomes less painful for the patient. For this purpose, it is recommended to use replaceable, sharp, single-use cannulas that are as thin as possible.
The neural therapy specialist physician performing neural therapy must learn to use the syringe and cannula with one hand. This procedure, which may seem routine, can lead to incorrect injections if not applied properly during daily neurotherapeutic procedures.
The syringe, a simple tool, not only enables the application of a local anesthetic substance to an anatomical structure, but also serves as a "sensor" for different tissues thanks to a sensitive injection technique.
SIDE EFFECTS AND RISKS OF NEURAL THERAPY
It is important to inform the patient not only about the risks, but also about the meaning of the injections. Regarding injection-related pain, the patient should be told, for example, that there may be lightning-strike-like pain during injection into peripheral nerves.
During the injection, attention should be paid to the patient's feedback regarding pain, because this feedback can be a sign that the needle is in the wrong position. Severe pain should not occur during any injection. In such cases, the injection procedure should be stopped and the position of the needle should be checked and corrected.
As a basic rule, every patient should remain under medical observation as much as possible, following neurotherapeutic treatment, for the duration of the effect of the local anesthetics used.
In addition to expected reactions such as dizziness, mild sensory disturbance, and brief loss of motor function, attention should also be paid to unexpected reactions such as vasovagal circulatory disorders and early allergic reactions.
COMPLICATIONS OF NEURAL THERAPY
Complications should never be entirely disregarded.
Every complication that occurs during treatment should be recorded.
INTRAVASCULAR (INTRA-ARTERIAL) INJECTION
Injection of a local anesthetic substance into a blood vessel is a rare but serious complication requiring emergency medical intervention.
The cause of this complication is generally that the double aspiration technique, together with the 180° needle rotation procedure, has not been performed correctly.
ANAPHYLAXIS
Anaphylaxis, which is very rarely seen, is independent of injection technique and requires emergency intervention under hospital conditions.
BLEEDING / HEMATOMA
Hematomas are among the complications that, depending on their location and spread, require either conservative treatment or, very rarely, surgical intervention.
During conservative neural therapy for a hematoma, repeated infiltrations with procaine are applied at as early a stage as possible in order to achieve faster resorption and infection prophylaxis.
ORGAN INJURIES
In organ injuries caused by the needle (e.g., lung, kidney, liver), surgical intervention is generally not required.
However, in cases of suspicion, the person should be kept under hospital observation.
These complications can occur not only due to injection errors, but also due to anatomical and topographical variations.
SPINAL DURA MATER PUNCTURE
Accidental puncture of the spinal dura mater during peridural infiltration is a rarely seen complication. This complication is seen more during spinal or paraspinal anesthesia procedures rather than in neural therapy applications.
This complication is thought to often cause post-spinal headache lasting several days.
 LOCAL ANESTHESIA DOSE IN NEURAL THERAPY APPLICATIONS
LOCAL ANESTHESIA DOSE IN NEURAL THERAPY APPLICATIONS
The maximum dose of a 1% procaine solution is 500 mg (50 ml of 1% solution) for extravascular application.
Such a high amount is never necessary in neural therapy applications.
The upper limit is 15-30 ml per session, and there is no need to exceed this amount.
If it is necessary to exceed this limit in some cases, it is appropriate to leave a gap of about ½-1 hour between the first and second injection.
During treatment, the goal should be to deliver procaine to the diseased tissue in as low a dose as possible, using a careful injection technique.
Exposing the tissue to an excessive amount of procaine should actually be regarded as a preventable error.
- Nazlikul, H: Neuraltherapie – Nobel Kitabevleri 2010 Istanbul
- Nazlikul, H: Neuraltherapie – Another Treatment Is Possible – Destek Yayınları 2019
- Nazlikul, H: Dissertation (Doktor medicinae) im Rahmen des postgradualen Universitätslehrganges für Ganzheitsmedizin –Regulationsmedizin "Neuraltherapie Naturheilverfahren, Regulationsverfahren und Herdgeschehen" von PD. Dr. med. Hüseyin Nazlikul 2010 Die Medizinische Fakultät Charité.
- Nazlikul, H.: Thorakale Wirbelblockaden erfolgreich therapieren S34-38, 1, 2/2008 für Allgemeinärzte
- Nazlikul H, Babacan A. Nöralterapi ve enjeksiyonlardaki rolü. Babacan A, editör. Ağrı ve Enjeksiyonlar. 1. Baskı. Ankara: Türkiye Klinikleri; 2019. p.110-7.
- Reuter URM, Oettmeier R and Nazlikul H (2017) Procaine and Procaine-Base-Infusion: A Review of the Safety and Fields of Application after Twenty Years of Use.
- Herget, F, H, Nazlikul, H: „Neurophysiologie und Neuropharmakologie der Schmerzmatrix" S. 56 ff
- J. Cassuto et al.;Antiinflammatory properties of local anesthetics and their present and potential clinical implications; Acta Anaesth Scand 2006 ;50:265-82
- M.W.Hollman et al; Local Anesthetic effects on priming and activation of human neytrophils; Anesthesiology 2001:95:113-22
- Barop, H.: Lehrbuch Neuraltherapie, Haug Verlag 1996
- Barop, H.: Lehrbuch Neuraltherapie, 2. Überarbeitet Auflage Haug Verlag 2015
- Fischer, L: Neuraltherapie nach Huneke 2004 HD